ABSTRACT
Hypertension is a highly prevalent issue worldwide. The prevalence of underdiagnosed hypertension in India calls for the need for this consensus article, which aims to optimize screening strategies. In this article, a modified Delphi approach was used to develop consensus statements. Key recommendations include the adoption of standardized screening protocols across diverse healthcare settings, incorporating both office-based and out-of-office blood pressure measurements (OBPM). By implementing these evidence-based strategies, the consensus aims to improve the early detection of hypertension, ultimately reducing the burden of cardiovascular disease and enhancing patient outcomes.
How to cite this article
Hiremath J, Wander G, Dasbiswas A, et al. Optimizing Screening Strategies for Hypertension in India: A Consensus Statement. J Assoc Physicians India 2025;73(4):e40-e46.
INTRODUCTION
Hypertension is a rampant global health condition, affecting around 1.28 billion adults aged 30–79 years, with a significant majority, two-thirds, residing in low- and middle-income countries. Alarmingly, approximately 46% of hypertensive adults remain unaware of their condition, underscoring a critical gap in diagnosis and management. 1 In India’s National Family Health Survey Fifth Series (NFHS-5), conducted between 2019 and 2021 and encompassing 1.7 million respondents, 28.1% were found to have hypertension. 2 A majority (~58%) of existing hypertension cases in India are undiagnosed, as per the current round of the NFHS. Different sets of international guidelines have different classifications and gradings of hypertension ( Table 1 ).
Classification of hypertension according to major guidelines
| InSH 2023 4 | ESH/ECC 2024 32 | AHA 2017 12 | |
|---|---|---|---|
| Normal | Not mentioned | <120/80 mm Hg | <120/80 mm Hg |
| Optimal | <130/85 mm Hg | 120–129/84–89 mm Hg | Not mentioned |
| Elevated | Not mentioned | Not mentioned | 120–129 mm Hg/<80 mm Hg |
| High normal | 130–139/85–89 mm Hg | 130–139/85–89 mm Hg | |
| Stage 1 hypertension | 140/90 mm Hg | 140–159/90–99 mm Hg | 130–139/80–89 mm Hg |
| Stage 2 hypertension | >160/100 mm Hg | 160–179/100–109 mm Hg | >140/90 mm Hg |
| Stage 3 hypertension | Not mentioned | >180/110 mm Hg | Not mentioned |
Early screening could reduce the morbidity and mortality linked to hypertension. Mass screening entails assessing healthy populations in public settings, such as markets, irrespective of individual risk factors. Targeted screening involves evaluating specific groups identified as having an elevated risk of hypertension compared to the general population. Opportunistic screening is conducted when individuals interact with the healthcare system or other environments where screening is available, such as human immunodeficiency virus (HIV) clinics or corporate health events. 3
According to the Indian guidelines, all adults aged 18 and above should undergo opportunistic screening at healthcare facilities during visits or as requested separately. 4
There are three techniques of blood pressure measurement: office blood pressure measurement (OBPM), ambulatory blood pressure measurement (ABPM), and home blood pressure measurement (HBPM). OBPM, or conventional in-office blood pressure, is measured at an office or in a screening setting using a sphygmomanometer. ABPM is measured over 24 hours, and HBPM, or self-measured blood pressure, is done at home or by the patient. 5
In India, around 20 crore adults are estimated to have hypertension, but only about 2 crore individuals have their condition under control. To address this issue, the Ministry of Health and Family Welfare, together with the Indian Council of Medical Research, state governments, and WHO-India, has initiated a 5-year program known as the Indian Hypertension Control Initiative (IHCI). As part of its commitment to combating noncommunicable diseases (NCDs), the Government of India has embraced the “25 by 25” target, which seeks to lower premature deaths from NCDs by 25% by the year 2025. Among the nine voluntary objectives is a goal to achieve a 25% decrease in the prevalence of hypertension by 2025. 6
NEED FOR CONSENSUS
Hypertension, often termed the “silent killer,” is frequently asymptomatic, leading to underdiagnosis and undertreatment. A national survey conducted between 2019 and 2021 involving 1.7 million respondents revealed that 28.1% had hypertension. However, only 36.9% of these individuals received a diagnosis, and a mere 44.7% of those diagnosed reported taking antihypertensive medication. It is important to note that only 52.5% of those on medication achieved blood pressure (BP) control, representing just 8.5% of the total hypertensive population. 2 These statistics highlight the critical need for enhanced screening protocols and effective management strategies to address the hypertension epidemic. A consensus on effective screening strategies is crucial to implementing a uniform, evidence-based approach that maximizes early detection and management of hypertension across diverse populations in India.
METHODOLOGY
A modified Delphi process was used to construct the consensus statements. 7 A group of 532 cardiologists, endocrinologists, and consulting physicians participated in the voting process held across 18 meetings in different cities in India.
Relevant literature was reviewed with a specific focus on Indian data whenever accessible. Following the review, statements were voted on electronically to ensure anonymity. The voting options provided were: accept completely, accept with some reservations, reject with reservations, accept with major reservations, and reject completely ( Fig. 1 ).
Methodology of consensus

A statement was classified as accepted if 75% or more of the voting members selected either “completely accept” or “accept with some reservations.” Similarly, a statement was regarded as refuted if 75% or more of the participants opted for “completely reject” or “reject with some reservations.” Finally, for statements that were accepted, participants evaluated the level of evidence and the strength of recommendation using a scheme adapted from the Canadian Task Force on the Periodic Health Examination ( Table 2 ). 8
Quality and strength of evidence
| Quality of evidence | Strength of evidence | ||
|---|---|---|---|
| Grade | Description | Grade | Description |
| I | Evidence obtained from at least one RCT | A | There is good evidence to support the statement |
| II-1 | Evidence from well-controlled trials without randomization | B | There is fair evidence to support the statement |
| II-2 | Evidence from a well-designed cohort or case-control study | C | There is poor evidence to support the statement |
| II-3 | Evidence from the comparison between time or place with or without intervention | D | There is fair evidence to refute the statement |
| III | Opinion of experienced authorities and expert committees | E | There is good evidence to refute the statement |
CONSENSUS STATEMENTS FOR SCREENING OF HYPERTENSION
The Primary Reason for Poor Hypertension Control is Underdiagnosis
Voting: 88%
LoE: II-3
SoR: D
Evidence: A cross-sectional analytical study conducted among adults visiting the outpatient departments of rural and urban health centers in a district of South India between May and December 2021 found that 199 (36.9%) had undiagnosed hypertension. According to the current round of the NFHS-5, approximately 58% of existing hypertension cases in India are undiagnosed. 2 A study using data from the 2017–2018 Longitudinal Aging Study in India found that 22.6% of adults aged 45 and above with hypertension remained undiagnosed, even after visiting healthcare facilities in the past year. If diagnosed, the prevalence of hypertension diagnosis would rise from 54.8 to 77.3%. 9 This highlights the need to optimize screening strategies in India.
Every Individual above 30 Years of Age Should be Screened for Hypertension
Voting: 92.0%
LoE: I
SoR: A
Evidence: The US Preventive Services Task Force mentions that yearly screening is recommended for adults aged 40 and above, as well as for individuals at higher risk of developing high blood pressure. High-risk groups include those with high-normal blood pressure (130–139/85–89 mm Hg) and individuals who are overweight or obese. 10 The Indian Society of Hypertension (InSH) recommends that all adults above 18 should undergo opportunistic screening by healthcare providers at all points of care in India. 4
Opportunistic Screening of Hypertension is Recommended for All Adults Irrespective of Risk Factors
Voting: 92.3%
LoE: II-3
SoR: D
Evidence: Opportunistic screening is conducted when individuals interact with the healthcare system or other environments where screening is available, such as HIV clinics or corporate health events. Opportunistic screening was conducted at a primary health center in rural Puducherry, screening a total of 324 participants, of whom 56.8% were female. Hypertension was present in 17.9% of the participants, while 37.7% had prehypertension. Generalized obesity was observed in 31.8% of participants, 45.1% had central obesity, and 19.1% were overweight. These findings highlight a significant prevalence of prehypertension and obesity, underscoring the importance of early intervention to manage these health risks. 11 Opportunistic screening in hospital settings serves as an effective technique to identify hypertension in otherwise healthy individuals and increase awareness among the population.
The Longitudinal Aging Study (2017–2018) in India also found that missed diagnoses were more common among poorer, less educated, male, rural, Hindu, living alone, and working individuals, and more frequent in private health facilities. Rates varied widely across states. Opportunistic hypertension screening could enhance detection and reduce sociodemographic and geographic disparities. 9
For Individuals below 65 Years of Age, It is Advised to Maintain Blood Pressure Levels <140/90 mm Hg
Voting: 85.0%
LoE: I
SoR: A
Evidence: According to the American College of Cardiology/American Heart Association (ACC/AHA) guidelines, optimal blood pressure levels for adults are 120/80 mm Hg. Hypertension is diagnosed only when blood pressure levels exceed 140/90 mm Hg, according to Indian guidelines and the European Society of Cardiology/European Society of Hypertension (ESC/ESH). 4 , 12 - 14 The ESH hypertension guideline recommends initiating treatment for DBP ≥90 or SBP ≥140 mm Hg, with the goal of achieving a target BP level below 130/80 mm Hg, particularly for individuals under 65 years of age. 13
For an Individual above 80 Years of Age, It is Recommended to Target Blood Pressure of <120/80 mm Hg
Voting: 7.4%
LoE: NA
SoR: NA
Evidence: ACC/AHA recommends a target of <130/80 mm Hg, whereas ESH recommends <140–150/80 mm Hg for adults over 80 years of age. 12 , 13
Blood Pressure is to be Lowered if ≥140/90 mm Hg and Treated to a Target <130/80 mm Hg in Patients with Hypertension with Coronary Artery Disease
Voting: 91.0%
LoE: I
SoR: A
Evidence: There is a significant epidemiological link between coronary artery disease and hypertension, contributing to 25–30% of acute myocardial infarctions. 15 According to the SPRINT study, a target BP of <130/80 mm Hg is recommended for patients with cardiovascular disease, such as coronary artery disease, heart failure, abdominal aortic aneurysm, peripheral artery disease, or left ventricular hypertrophy. 16
In a study conducted by Huang et al. (2017), the ideal achieved BP for ethnic Chinese patients with stable CAD in Taiwan was investigated. The study included 2,045 patients with stable CAD who had previously undergone percutaneous coronary interventions. The study found that SBP below 120 mm Hg or above 160 mm Hg, as well as DBP below 70 mm Hg, were linked to a higher risk of cardiovascular events. The findings suggest that optimal BP control should be carefully managed for stable CAD patients in non-Western populations. 17
Blood Pressure is to be Decreased if ≥140/90 mm Hg and Treated to a Target of <130/80 mm Hg in Patients with Hypertension with Previous History of Stroke
Voting: 84.3%
LoE: I
SoR: A
Blood Pressure to be Decreased if ≥140/90 mm Hg and Treated to a Target <130/80 mm Hg in Patients with Hypertension with Acute Stroke
Voting: 37.7%
LoE: NA
SoR: NA
Evidence: A randomized clinical trial assessed the effects of intensive BP control (target <120/80 mm Hg) vs standard control (<140/90 mm Hg) in patients with a history of stroke. A total of 1,263 patients were assigned to standard treatment ( n = 30) or intensive treatment ( n = 33). The trial found a nonsignificant reduction in stroke recurrence with intensive BP control (HR 0.73, 95% CI 0.49–1.11). However, when pooled with three other RCTs in a meta-analysis (total n = 4,895), intensive BP control significantly favored stroke prevention (relative risk 0.78, p = 0.02). The findings support targeting BP <130/80 mm Hg for secondary stroke prevention. 18
According to Canadian guidelines, for patients with a history of ischemic stroke or transient ischemic attack, blood pressure-lowering treatment is advised to achieve a target consistently lower than 140/90 mm Hg. 19 InSH 2023 recommends that blood pressure should be lowered if it is ≥140/90 mm Hg, with a treatment goal of reducing it to <130/80 mm Hg in patients with hypertension who have a history of stroke. AHA 2017 and ISH 2020 recommend a BP-lowering goal of <130/80 mm Hg for those with a stroke or transient ischemic attack. 12 , 15
Blood Pressure to be Decreased if ≥140/90 mm Hg and Treated to a Target of <130/80 mm Hg in Patients with Hypertension with Chronic Kidney Disease
Voting: 86.8%
LoE: I
SoR: A
Evidence: The 2017 American College of Cardiology/American Heart Association guidelines recommend a target of <130/80 mm Hg. The European Society of Cardiology/European Society of Hypertension recommends SBP of 130–139 mm Hg, while the 2019 hypertension guideline from the National Institute for Health and Care Excellence recommends <140/90 mm Hg. 12 , 13 , 20 Kidney Disease: Improving Global Outcomes (KDIGO) 2024 recommends an SBP treatment target of <120 mm Hg in CKD patients. 14
A study by Gentile et al. critically appraised existing evidence and key international guidelines regarding blood pressure management in patients with chronic kidney disease and hypertension. It concluded that clinicians should aim for a BP target lower than 130/80 mm Hg in these patients, except for those who were frail or had multiple comorbidities. 13
Blood Pressure to be Lowered if ≥140/90 mm Hg and Treated to a Target <130/80 mm Hg but >120/70 mm Hg in Patients with Hypertension with Heart Failure
Voting: 77.2%
LoE: I
SoR: A
Evidence: A meta-analysis found that blood pressure control was linked to a roughly 40% decrease in HF events. 21 A post hoc analysis identified that an SBP target of <130 mm Hg was associated with reverse remodeling and improved cardiac function in patients with subclinical hypertensive heart disease. 22
The 2022 ACC/AHA guidelines recommended a target of <130/80 mm Hg for hypertensive patients at high risk of HF, as well as those with clinical HF. 23 This target aligns with the recommendations in the latest hypertension guidelines from India, China, and Japan ( Table 3 ). 4 , 24 , 27
BP cutoffs by different guidelines in different comorbidities
| Condition | InSH 2023 | ESH 2024 | ACC/AHA 2017 | ISH 2020 |
|---|---|---|---|---|
| CAD | 140/90 mm Hg | 130/80 mm Hg | 130/80 mm Hg | 140/90 mm Hg |
| Previous stroke | 130/90 mm Hg | 130/80 mm Hg | 130/80 mm Hg | 130/80 mm Hg |
| CKD | 140/90 mm Hg | 130/80 mm Hg | 130/80 mm Hg | 140/90 mm Hg |
| HF | 140/90 mm Hg | Specific target not mentioned | 130/80 mm Hg | 140/90 mm Hg |
ACC/AHA, American College of Cardiology/American Heart Association; CAD, coronary artery disease; CKD, chronic kidney disease; HF, heart failure; InSH, Indian Society of Hypertension; ISH, International Society of Hypertension
Home Blood Pressure Should be Checked for 7 (Not Less than 3) Days with Duplicate Morning and Evening Measurements before Office Visits
Voting: 90.8%
LoE: I
SoR: A
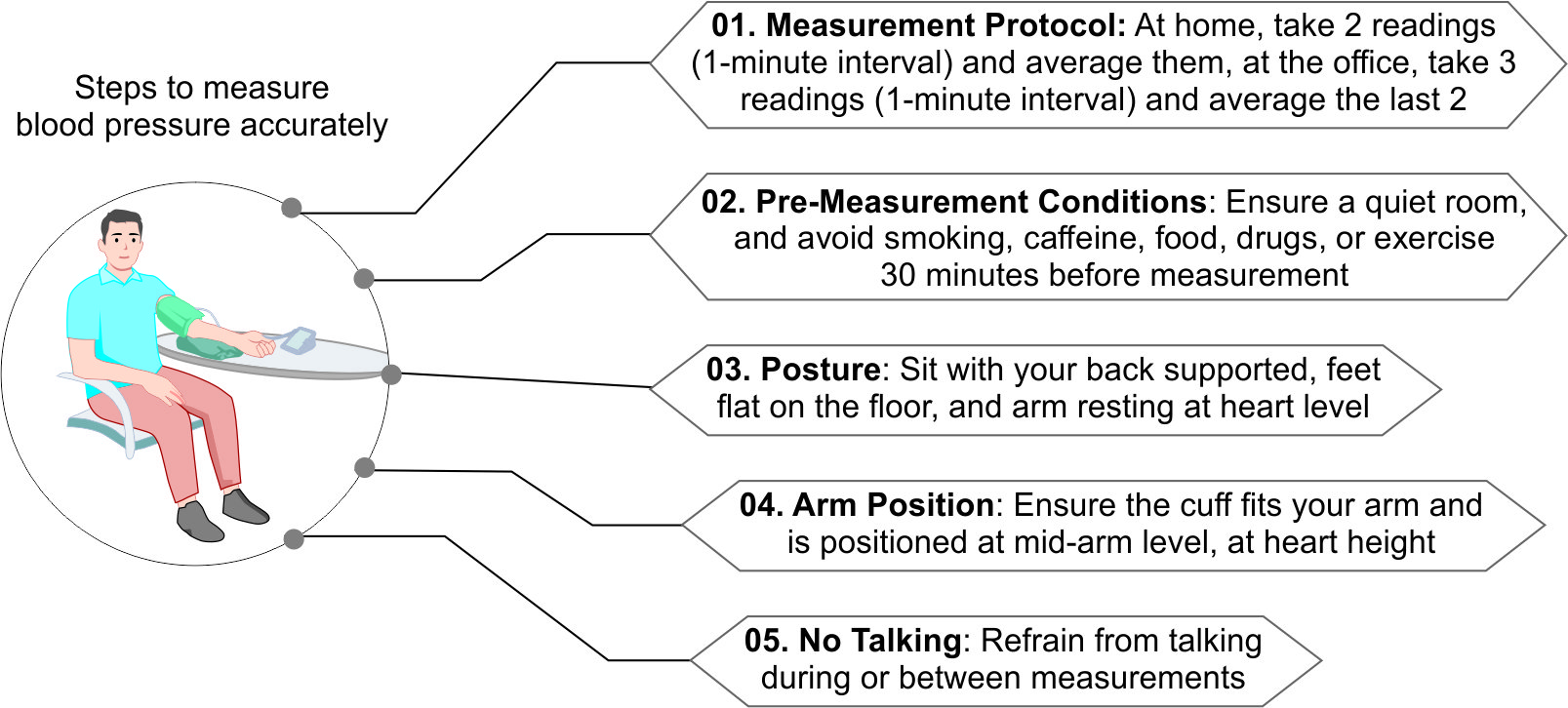
Evidence: The ESH guidelines recommend monitoring HBP for 7 days, or at least 3 days if 7 days is not possible, with measurements taken twice each time, 1 minute apart, in the morning (before taking any medication if treated) and in the evening. It is recommended to monitor blood pressure before scheduled office visits or whenever there is a noticeable change in blood pressure. 13
A survey conducted between June 2020 and June 2021 among 832 Indian physicians revealed that while 88% of those managing hypertensive patients recommend HBPM, only 34.9% of patients own an HBPM device and 30.4% use it regularly. Instructions for HBPM are inconsistent and often not aligned with local guidelines, suggesting a need for improved educational resources for physicians as well as patients. 26
Primary care physicians countrywide in Greece were invited to participate in a cross-sectional study by Kollias et al. involving 790 hypertensive patients. HBP was measured over 7 days with repeated morning and evening readings, showing that office blood pressure (OBP) measurements (137.5/84.3 mm Hg) were significantly higher than HBP measurements (130.6/79.9 mm Hg). This method revealed that 22.7% of patients had white-coat hypertension (WCH), while 15.8% had masked uncontrolled hypertension (MUCH). By identifying these conditions, HBP monitoring helps avoid overtreatment in WCH patients and ensures proper treatment for those with MUCH, ultimately preventing excess cardiovascular disease and improving patient outcomes ( Fig. 2 ). 27
Steps to for accurate BP measurement
Ambulatory Blood Pressure Monitoring is Suggested to Identify Masked Hypertension, White-Coat Hypertension and Nocturnal Blood Pressure Phenotypes
Voting: 91.8%
LoE: I
SoR: A
Evidence: Ambulatory blood pressure monitoring (ABPM) involves continuous blood pressure measurement, usually over a 24-hour period, to evaluate fluctuations in blood pressure patterns. This method offers a more accurate assessment of true blood pressure compared to standard one-time measurements. ABPM can identify circadian patterns, such as diurnal rhythms, nocturnal dipping, and morning surges, as well as variations due to environmental and emotional factors. 28 About 10–20% of patients visiting hypertension clinics have masked hypertension. 13 In a study conducted across 10 populations in Asia, Europe, and South America, it was found that masked hypertension had a prevalence of 16.9% in 2017. 29
Nighttime hypertension is identified as an average BP ≥120/70 mm Hg recorded during the night hours with ABPM. 13 According to the ACC/AHA 2017 guidelines, a normotensive patient should have a daytime ABPM reading of <120/80 mm Hg and a nighttime ABPM reading of <100/65 mm Hg ( Tables 4 and 5 ). 12
Guidelines recommendations on HBPM and ABPM
| 2023 Indian Guidelines on Hypertension 4 | 2023 ESH Guidelines 33 | 2017 ACC/AHA Guidelines 12 | 2024 ESC Guidelines 32 | |
|---|---|---|---|---|
| HBPM | Recommended for long-term follow-up of treated hypertension | ABPM may have a stronger prognosis, utility in nocturnal monitoring, and better representativeness in real-life settings than HBPM | Out-of-office measurements, that is, ABPM and HBPM, over office measurements for confirming diagnosis and monitoring BP control | Recommended for long-term follow-up of treated hypertension |
| ABPM | Recommended to identify white-coat hypertension, masked hypertension, and nocturnal BP phenotypes Repeated ABPM may be required because these phenotypes have limited reproducibility | More accessible and comfortable for the patient | Obtaining a 24-hour BP profile not captured by office BP measurement or HBPM |
ABPM, ambulatory blood pressure monitoring; HBPM, home blood pressure monitoring
HBPM and ABPM cutoffs mentioned in different guidelines
| ESH 2024 | ACC/AHA 2017 | InSH 2023 | |
|---|---|---|---|
| HBPM | 135/80 mm Hg | 135/80 mm Hg | – |
| ABPM-24-hour mean | 130/80 mm Hg | 130/80 mm Hg | – |
| Nighttime | 120/70 mm Hg | 120/70 mm Hg | – |
| Daytime | 135/85 mm Hg | 135/85 mm Hg | – |
ABPM, ambulatory blood pressure monitoring; ACC/AHA, American College of Cardiology/American Heart Association; ESH, European Society of Hypertension; HBPM, home blood pressure monitoring; InSH, Indian Society of Hypertension
Every Patient Must Do All Necessary Lab Investigations Every Six Months to Rule Out Hypertension-mediated Organ Damage
Voting: 74%
LoE: NA
SoR: NA
Evidence: According to InSH 2023, to optimize cardiovascular and kidney risk assessment, it is recommended that hypertension-mediated organ damage (HMOD) be evaluated as soon as hypertension is diagnosed. This evaluation can guide decisions about initiating or adjusting treatment. Basic screening for HMOD should be performed in all hypertensive patients, with more detailed assessments when HMOD is critical for treatment decisions. Routine tests for detecting HMOD in hypertensive patients include serum creatinine and eGFR, calculated using the CKD-EPI formula. A 12-lead ECG is also recommended to assess cardiovascular health. Additionally, the urine albumin-to-creatinine ratio should be measured, or alternatively, the urine protein-to-creatinine ratio or urine albumin, if necessary. If available, Cystatin C may be used for the early detection of nephropathy ( Table 6 ). 4
Final expert recommendations
| 1. | The primary reason for poor hypertension control is underdiagnosis |
| 2. | Every individual above 30 years of age should be screened for hypertension |
| 3. | Opportunistic screening of hypertension is recommended for all adults irrespective of risk factors |
| 4. | BP is to be lowered if ≥140/90 mm Hg and treated to a target <130/80 mm Hg in patients with hypertension with coronary artery disease (CAD) |
| 5. | For individuals under 65 years of age, it is advised to maintain blood pressure levels <140/90 mm Hg |
| 6. | BP is to be decreased if ≥140/90 mm Hg and treated to a target of <130/80 mm Hg in patients with hypertension with previous history of stroke |
| 7. | BP to be decreased if ≥140/90 mm Hg and treated to a target of <130/80 mm Hg in patients with hypertension with chronic kidney disease (CKD) |
| 8. | BP to be decreased if ≥140/90 mm Hg and treated to a target <130/80 mm Hg but >120/70 mm Hg in patients with hypertension with heart failure (HF) |
| 9. | Home BP should be checked for 7 (not <3) days with duplicate morning and evening measurements before office visits |
| 10. | ABPM is advised to identify white-coat hypertension, masked hypertension and nocturnal BP phenotypes |
| 11. | It is suggested to use longer acting drugs (≥24 hours) to prevent morning surge of BP |
It is Suggested to Use Longer Acting Drugs (≥24 hours) to Prevent Morning Surge of Blood Pressure
Voting: 86.0%
LoE: I
SoR: A
Evidence: A comparative study found that amlodipine reduced ambulatory BP more effectively than nifedipine gastrointestinal therapeutic system, achieving reductions of 22.6/12.6 mm Hg vs 17.7/11.4 mm Hg over 24 hours. The most significant variations were observed during the early morning hours (5–10 AM). 30 Furthermore, the VALUE trial found that valsartan was less effective than amlodipine in managing blood pressure during the morning trough period, showing a systolic BP difference of approximately 3 mm Hg. These findings indicate that even once-daily antihypertensive medications can show significant variations in 24-hour BP control, particularly in the early morning. Among five guideline-recommended classes—telmisartan, perindopril, bisoprolol, amlodipine, and chlorthalidone—those with the longest biological half-lives may offer extended BP-lowering effects. 29
Aneroid, or Cuffless Automated Blood Pressure Devices Should be Used and Preferred in Clinical Practice
Voting: 37.6%
LoE: III
SoR: E
Evidence: The mercury sphygmomanometer and the aneroid variety are no longer recommended by WHO. 31 However, according to ESH 2023 guidelines, cuffless BP devices are not currently recommended for the management or diagnosis of hypertension in clinical practice. However, ESH suggests the use of mercury sphygmomanometers, aneroid sphygmomanometers, hybrid devices with LED or LCD displays, automated oscillometric devices (including wrist cuff models), automated auscultatory devices, and semiautomated devices. “The automated cuff-based BP measurement method (primarily oscillometric) has been developed to eliminate observer-related errors associated with the manual auscultatory technique.” 13
CONCLUSION
This consensus emphasizes the importance of comprehensive screening strategies for hypertension to address the critical issue of underdiagnosis. Opportunistic screening for all adults is recommended, with a focus on achieving a target BP of <130/80 mm Hg in high-risk populations, including those with CAD, stroke history, CKD, and HF. Home BP monitoring and ABPM are advised to accurately assess BP and identify conditions like white-coat and masked hypertension. These strategies aim to enhance hypertension control and improve patient outcomes.
FUNDING
Funding for medical writing support was provided by Alembic Pharmaceuticals Ltd.
CONFLICT OF INTEREST
Dr Onkar Swami, Dr Sanjay Jain, and Dr Priyank Shah are full-time employees of Alembic Pharmaceuticals Ltd., which actively markets antihypertensive drugs.
ACKNOWLEDGMENT
The authors would like to thank Intellimed Healthcare Solutions Pvt. Ltd. for their assistance in medical writing.
ORCID
Mahesh K Shah https://orcid.org/0000-0001-8879-9504
D Prabhakar https://orcid.org/0000-0003-2218-5862
Onkar Swami https://orcid.org/0000-0001-6006-7520
REFERENCES
ARTICLE INFO
Publication history
received: 03 February, 2025
accepted: 17 February, 2025
Published: 01 April, 2025
Copyright
Copyright © 2025; The Author(s).